
Update: May 5, 2021 The U-turn is official.
Sweden has officially ended the practice of prescribing puberty blockers and cross-sex hormones for minors under age 18. They have recognized the experimental nature of treating minors with puberty blockers and hormones and have established new protocols that deviate significantly from WPATH and the “professional associations” that the Canadian government and healthcare authorities are listening to. You can access the official documents and read more at the summary published by the Society for Evidence-based Gender Medicine.
Original post:
Is Gender Transition Medically Necessary?
The graph below shows all referrals to gender clinics in Sweden. The inverted U shape of the curve is extremely interesting. Referrals to gender clinics fell off a cliff in 2019. Why? And why no rebound? Does the Swedish experience tell us something about the hype and potential disillusionment surrounding the practice of medically transitioning children?
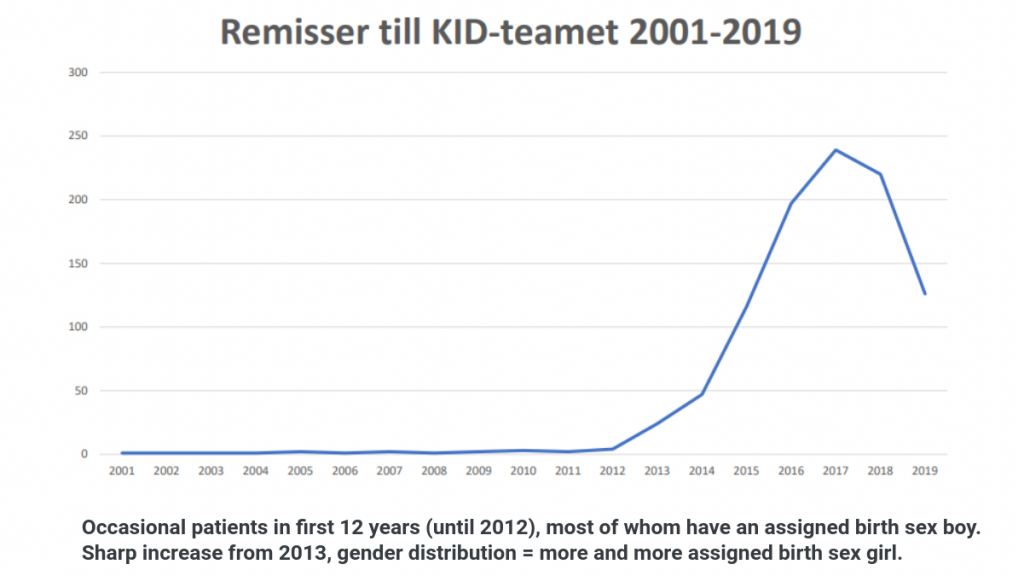
Source: Presentation by Louise Frisén, Chief Physician, Associate Professor of Child and Adolescent Psychiatry at the KID (Stockholm) clinic for gender incongruence and gender dysphoria – delivered at a Swedish Medical Ethics Council Seminar February 6, 2020
The sudden, sharp increase suggests a triggering event. Certainly, the explosive growth in natal females seeking gender transition is a new phenomenon throughout high-income countries. It has coincided with the advent of social media and the popularisation of “transgenderism” in mainstream media and on-line.
Swedish child psychiatrist, Sven Roman has compared the explosive growth in the number of cases of gender dysphoria to other psychiatric conditions, such as eating disorders and self-harm behaviour, that are known to spread with social contacts. He documents the process of discovery that the medical community went through to understand how to best treat these kinds of conditions. Over the past decade, he says research has proven that supportive psychotherapy can reduce or stop self-harm behaviour within 3 months. Of the avalanche of gender dysphoria cases being referred, he says:
Unlike the epidemic of self-harm behavior, (gender dysphoria) care providers are not exploring to find the right treatment. Instead, on a broad front, drastic treatment with high doses of sex hormones and breast and genital surgery is introduced. This despite the lack of any scientific evidence for these treatments for children, and probably not for young adults either.
Sven Roman, MD and child psychiatrist
In the fall of 2019, there was a 65% decline in the number of referrals to gender clinics in Sweden. This corresponded with experts calling on the government to review clinical protocols and more balanced media coverage of the phenomenon of regret among gender transitioners, including the airing of a documentary entitled “Trans Train”.
The 3-part documentary includes several interviews with detransitioners and revealed that medical transition of minors is not evidence-based. A high profile transwoman in Sweden – Aleksa Lundberg – also came out in the media saying that if she were to go back and make the decision again “I might not have had the surgery”. She said she had believed that “there was a more scientific basis” for this healthcare – but has since realized that that is not the case. She says people deserve “a more complex narrative” than the simple public narrative that the media has been promoting on the topic of gender transition.
Referrals have remained steadily lower, indicating that the medical necessity of gender transition was questionable for many of the youth being referred for treatment. We are told that the treatment of minors now (unofficially) includes referring many to psychiatric evaluation. Previously, we are told that almost 100% of trans-identified youth who were referred to the gender clinics were prescribed puberty blockers or cross-sex hormones.
Some Background
In the fall of 2018, Sweden’s Social Democrat government proposed a new law that would have reduced the minimum age for sex reassignment surgery from 18 to 15, remove any need for parental consent and allow children as young as 12 to change their legal gender.
The government received a major backlash from the scientific community, however. Christopher Gillberg, a professor and psychiatrist at Gothenburg’s Sahlgrenska Academy, wrote an article in the Svenska Dagbladet newspaper warning that hormone treatment and surgery on children was “a big experiment” which risked becoming one of the country’s worst medical scandals.
The Swedish government shelved their proposed law and instead, have instituted a 3 part review in response to a proposal from The Swedish National Council on Medical Ethics.
Ongoing Review Tasks Three Government Agencies
In late 2019, the Swedish National Council on Medical Ethics proposed that the Ministry of Health and Social Affairs task three government agencies to “strengthen the knowledge base for the assessment and treatment of gender dysphoria among children and adolescents”. They outlined their concerns as follows:
In our dialogues with stakeholders, we have encountered widely differing views on the assessment and treatment of gender dysphoria, which also characterizes the specialist literature and public debate. These differences are partly about the facts and how they should be interpreted, and partly about values.
And
Irrespective of their attitude to health care activities in this area, the actors make it clear that the scientific basis needs to be strengthened. When the Swedish National Council on Medical Ethics has discussed ethical issues regarding gender dysphoria, knowledge gaps and uncertain knowledge has been a central theme.
In their letter, three government agencies were highlighted as needing to participate:
- The Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU) – to undertake a systematic literature review of the scientific basis used for assessing children and young people with gender dysphoria, and what is known about the long-term effects on physical and mental health. This should also include a review of what is known about the causes of the increase in the number of children and young people, particularly girls, seeking assessment and treatment for gender dysphoria in high-income countries. Differing claims about how common it is for people, who have begun treatment for gender dysphoria as children or adolescents, to change their minds, occur in the debate. What is known about this should also be included in the review.
- The Swedish Medical Products Agency – to analyse the off label prescription of puberty blockers and hormones to children and young people.
- The National Board of Health and Welfare should be instructed to urgently update its knowledge support material entitled ´God vård av barn och ungdomar med könsdysfori´ (‘Good care for children and adolescents with gender dysphoria’).
Sweden National Board of Health and Welfare Update
The NBHW are revising their treatment guidelines, to be distributed for comments to organisations and the public during 2021 and finalised 2022.
Officially and to date, the National Board of Health and Welfare has only released a preliminary report on “The development of the diagnosis of gender dysphoria”: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2020-2-6600.pdf
The summary conclusions from that report state:
“The diagnosis of gender dysphoria is increasing in the population, especially among children and young adults, where the proportion of new cases among 13– 17-year-old adolescents registered as female at birth has increased most. The increased rate of new cases will lead to an increasing total number of people diagnosed with gender dysphoria. In light of this, the development will require that health care is appropriately designed and sufficiently robust to ensure comprehensive investigation and treatment. In addition, treatment can be lifelong, which means that people with gender dysphoria need support from the healthcare system for extended time periods. People with gender dysphoria, especially young people, have a high incidence of co-occurring psychiatric diagnoses, self-harm behaviors, and suicide attempts compared to the general population. Co-occurring psychiatric diagnoses among people with gender dysphoria are therefore a factor that needs to be considered more closely during investigation. Suicide mortality rates are higher among people with gender dysphoria compared to the general population. At the same time, people with gender dysphoria who commit suicide have a very high rate of co-occurring serious psychiatric diagnoses, which in themselves sharply increase risks of suicide. Therefore, it is not possible to ascertain to what extent gender dysphoria alone contributes to suicide, since these psychiatric diagnoses often precede suicide.”
Swedish news coverage of this report also reports that “the authority’s survey shows that people with gender dysphoria, especially young people, have a high incidence of concomitant psychiatric diagnoses, self-harming behavior or suicide attempts compared with the rest of the population.” Further, “The diagnoses that stand out are depression, anxiety disorders, ADHD and autism.”
In the group of 13–17-year-old natal females, the Swedish NBHW report states that the comorbidity is greatest. In this unprecedented cohort of teenaged girls seeking gender transition the following co-morbidities were found:
- 32.4 percent anxiety disorder
- 28.9 percent some form of depressive disorder
- 19.4 percent ADHD
- 15.2 percent autism
The report also raises important questions about causation and suicide risk for people with gender dysphoria given the “very high rate of concomitant difficult psychiatric diagnosis”. This makes it difficult to distinguish one from the other with regard to suicide risk, said an investigator at the National Board of Health and Welfare.
Current Treatment Protocol in Sweden
Sweden does not allow gender-affirming surgeries on youth under the age of 18.
According to a recent video, as of late 2020, only child psychiatric specialists are able to refer children to gender clinics for assessment that can lead to the initiation of puberty blockers or cross-sex hormone therapy. The country continues to seek additional evidence to support these care standards.
The review by the Swedish Agency for Health Technology Assessment and Assessment of Social Services has not found any evidence to explain the increase in prevalence of children and adolescents who seek gender transition and “few” studies on gender-affirming treatment. The review does not provide any opinions on the conclusions or methodology used in those studies. The summary of this review is available in English here:
Sweden’s Increase in Referrals to Gender Clinics Similar to Canada
Sweden had seen a 1,500% increase in referrals for gender transition between 2008 and 2018 according to data from Sweden’s Board of Health and Welfare. The increase in Sweden is being driven by youth 13-17 years old born female. This trend is consistent with the data reported by Trans Youth Can! – a group running a voluntary observational study on youth who have been referred for puberty blockers and other hormone therapies in Canada.
Conclusions
The fast-tracking of medical transition appears to be the protocol in place at many of Canada’s gender clinics, with parents and some detransitioners expressing surprise and shock that medical transition is being offered as the 1st line of treatment. The sharp drop-off in referrals in Sweden corresponded to the realization by parents and General Practitioners that sending children to a gender clinic would not necessarily provide them with additional assessment or services, but rather put them on a fast-track to puberty blockers and cross-sex hormones.
The experience in Sweden, and corresponding similarities in Canada, points to a significant gap in assessment and services for trans-identified youth to ensure that their long term physical and mental well-being is prioritized over and above a quick fix of puberty blockers and cross-sex hormones. Research indicates youth become trapped in a one-way medical path as almost 98% who are prescribed puberty blockers proceed with medical transition even when there is no evidence of long-term benefits.
Further, suicide risk is often used as the rationale for easy access to medical transition for trans-identified children and adults. Pro-transition advocates consider the need for assessments and screening to be dehumanizing and unnecessary. Clearly, the data from the Swedish NBHW does not support this position. People who commit suicide have an underlying mental illness that requires expert treatment and care. It would be medically negligent to avoid psychiatric assessment and/or deny corresponding psychological services to provide treatment for this population where the risk of suicide is elevated due to these comorbidities.
It will be very interesting to see how the official clinical guidelines in Sweden take shape and evolve over the next 2 years.
When will Canada start asking questions like Sweden?


What are the units for the graph and what is its source?
Thank you for the excellent question. The source of the chart is a presentation by Louise Frisén, Chief Physician, Associate Professor of Child and Adolescent Psychiatry at the KID (Stockholm) clinic for gender incongruence and gender dysphoria. This presentation was delivered at a Swedish Medical Ethics Council Seminar February 6, 2020
You may find it here:
http://www.smer.se/wp-content/uploads/2020/02/3.-Louise-Frisén.pdf
The units on the x axis are # of patient referrals > 18 years of age at the Stockholm gender clinic. We’ll update the article to include the source. Thank you for pointing out this oversight.
It seems that the transgender madness is beginning to be noticed by authorities and professionals. In good time. Let’s hope it’s not too late.
At least on the other side of the world. We still have work to do in Canada and the USA is a whole different matter. This new trend is big business down there.
Since publishing we’ve been made aware of an excellent article by Mikael Landén, Professor, University Hospital Chief Physician, Section of Psychiatry and Neurochemistry, Sahlgrenska Academy, University of Gothenburg
https://lakartidningen.se/klinik-och-vetenskap-1/kommentar/2019/10/okningen-av-konsdysfori-hos-unga-tarvar-eftertanke/
In this article (for which he won an award) he puts forward that “culturally-linked psychologial infection” (aka social contagion) is a possible explanation for the exponential increase in youth seeking gender transition. We’ll update our article with more info but he states:
An alternative is culturally bound psychological infection. If people in their early teens are encouraged to think about their gender identity and are taught that gender dysphoria is a normal variant, it is not unlikely that some young people will direct their identity search towards gender identity. Such a search can spread quickly in social networks, as described for a number of other phenomena such as bulimia, suicide (increases when famous people or someone you know has taken their life), smoking, obesity and more [8].
The increased use of social media coincides in time with the increase in gender dysphoria [9] and may have facilitated the spread of social networks. Autism spectrum disorders are more common in people with gender dysphoria [10], and it may be people who are more sensitive to such effects.
Gender care in Canada is already a slow and careful process. Youth need to go through a hormone readiness assessment than can take anywhere from weeks to years, depending on the complexity of the individual. The assessments are performed by doctors specializing in gender care. THEN they can seek puberty blockers (which don’t have long-term medical impacts if used according to regulations), or if they are older, cross sex hormone therapy. Surgery on minors is very rare.
Canada also doesn’t bother to provide meaningful or accessible mental health services to youth, so it’s disingenuous to imply that making gender affirming therapy harder to access would somehow lead to these youth receiving mental health support for their co-morbid mental health diagnoses. It won’t. You basically have to show up at an ER holding a rope to access even basic mental health support in Canada. And that’s if you are lucky enough to live in an urban centre that has the capacity to half-ass respond to an emergency.
You also conveniently left out the studies showing that access to gender affirming care in adolescence actually decreases suicidality over 70%, and depression by 60% (Tordoff, 2022). It seems odd to leave out these stats, given your stated concern about finding interventions that treat the comorbidities associated with gender dysphoria. It seems like you are looking for interventions that align with your political ideology more than you are intervention that are actually evidence-based and effective.
I thought that access to puberty blockers and hormones was a careful process as well until I started to meet parents whose children received prescriptions at their first visit to a clinic. This Canadian research recently found that 62% of children receive a prescription for puberty blockers or a cross-sex hormone at their first visit to a gender clinic. What assessments are happening in these first visits then? Clearly not a slow or careful process. https://publications.aap.org/pediatrics/article/148/5/e2020047266/181329/Transgender-Youth-Referred-to-Clinics-for-Gender
Also, the research on suicide is very problematic and there are no good quality studies that support the idea that gender medicalization (the result of gender affirming care in Canada) will reduce or prevent suicide. Suicide risk is a narrative that is used to promote access to gender medicalization, even when the risks of such interventions may outweigh the benefits. Suicidal ideation has been found to be elevated in young people who identify as transgender, but not moreso than young people suffering from mental health conditions but who do not have gender dysphoria. It is well known that death by suicide among young people who identify as transgender is very low: https://link.springer.com/article/10.1007/s10508-022-02287-7
Suicidality is a complex phenomenon and gender transition should not be viewed as suicide-prevention measure.
This might be of interest to readers of this website:
Dr. A. Hutchinson and Dr. M. Midgen are experienced clinicians who have both worked in the NHS Gender Identity Development Service for children and young people (GIDS).
The exponential rise in adolescent natal females (teenage girls) presenting at gender identity services over the last few years has been well documented. This phenomenon was noted first amongst professionals working in the field and latterly has been picked up by the press and the public. Back in November 2019, for example, Newsnight and radio 4 covered this issue. During the programme “Going back: The people reversing their gender transition” (File on Four, Radio 4, Tuesday 26/11/19) Dr. Elizabeth Van Horn (Consultant Psychiatrist in The Gender Identity Clinic, The Tavistock and Portman NHS Foundation Trust), in response to the question about this explosion in referrals of natal females presenting at the Gender Identity Development Service calmly remarked we ‘do not know’ what might be driving this rise.
This gave a surprising impression of a lack of curiosity, insight and experience on the part of current clinicians. We suggest, in contrast, that many others working in this field have been asking themselves this very question for several years. They have generated hypotheses to account for this noteworthy and concerning phenomenon and refute the claim that it arises solely out of reduced stigma and increased access to services.
We posit that there are multiple, interweaving factors bearing down on girls and young women that have collided at this particular time causing a distress seemingly related to gender and their sex. These factors comprise both the external world (i.e. the social, political and cultural sphere) and the internal (i.e. the emotional, psychological and subjective). The external and internal interact and feed each other [1].
It is notable that even speaking about these observable, and clinically relevant, factors are seen by some as evidence of a form of anti-trans rhetoric. This deeply disturbs the clinicians whose professional lives are dedicated to understanding the source and meaning of human distress. It is from this place that we speak.
In spite of apparent social gains for minority groups, our present-day culture obsesses in highly gendered ways over the signifiers of what it means to be a boy and a girl, a man and a woman. Girls are under ever more pressure to capitulate to the ‘pinkification’ and ‘pornification’ of girlhood. Girls who eschew these signifiers, who are uncomfortable or dissent from this demand, can often be lonely and isolated in their apparent idiosyncrasy. Sexual feelings awaken amidst sexual harassment and press reports of misogynist hate crimes. Dawning same-sex attraction can occur against a backdrop of homophobia; as well as a dearth of everyday, run-of-the-mill lesbian visibility. This is particularly relevant for girls drawn to an aesthetic which is viewed as ‘masculine’ (and therefore wrongly ascribed as ‘male’), but could be understood and owned as a butch lesbian identity if only these girls had access to it. Linked to this is the absence of critical feminist thought of the most elementary nature in the school curriculum. Failing that, even basic sex parity in the classroom would impact early on the sorts of messages both girls and boys internalise about their capacities and the expectations others have on them.
Changes to the body during puberty can bring about much more turmoil than is readily acknowledged. It is particularly disconcerting and shame-inducing for girls who begin menarche early, and have to navigate the whole mess and embarrassment of sanitary protection in primary school toilet provision often ill-equipped for this. There is embarrassment inherent in growing breasts, of these being noticed and pejoratively commented on and, worse, groped.
Crucially, it is important to acknowledge, that girls and young women have long recruited their bodies as ways of expressing misery and self-hatred. Bodies become the site onto which they can project their perceived failure to live up to society’s expectations of them and also their internal, psychic pain. Psychic pain that arises out of the manifold implications of being a suffering human being: trauma, abuse, neglect, bullying, social ostracism, bereavement to name but a few. Also, for some, the fear of leaving childhood behind, the terror of female adulthood, is overwhelming.
It is not unreasonable to hypothesise that developing gender dysphoria, and alighting on a trans identity as the way of understanding, can, in some instances, be the solution (cure) to the ‘problem’ of being born female. It could be the ultimate act of self-harm. A form of self-harm hardly noticeable to many because it is so aligned with the disavowed but ever present attack on gender non-conforming women that exists throughout society.
We cannot ignore the role of the internet in this; whether cyber bullying, competitive instagram, exposure to pornography, sexualisation or the associated phenomenon of a sort of social and collective influencing. We know that there is a parallel world of on-line engagement where children and young people are engaging globally out of sight of any mediating influence or alternative explanation for their distress.
Whatever influencing factors, both exogenous / social and endogenous / psychological, there might be these are all happening within the wider context of the decimation of local child and adolescent mental health services (CAMHS) over the last decade. We are seeing a generation of young people emerge who have been poorly served by local specialist provision: a phenomenon recognised and documented here.
In the clinical setting we have become familiar with narratives, especially in younger children, resting almost entirely on the most superficial of signifiers: toys, activities, hair, clothes, a certain aesthetic upon which effectively the (self) diagnosis of trans is made, and a social role transition affected. Unfortunately these tropes are compounded and perpetuated by some “diversity” trainings delivered in schools.
We have also witnessed a coincidence of autistic spectrum conditions and gendered/ sexed distress. The lens of gender can seem very apt for these girls retrospectively to understand their difficulties: always feeling weird, not fitting in, struggling to understand social interactions and cues, bullied often, feeling themselves to be outside the norm. Additionally girls struggle physically with puberty; as a change from the familiar, often unpredictable, body sprouting and changing, unwanted thoughts and feelings.
The distress of their body seems to accrue over time for these young females; it was not primary. Socially transitioning might even have an iatrogenic effect on gender dysphoria as the body becomes a shameful secret that needs to be disavowed – we see embodied disconnection and alienation snowball. We are now hearing first hand from detransitioners that, had they not found this relatively novel way of understanding their difficulties (inevitably with the assistance of the internet) through the explanation of ‘trans’, the natural history would suggest they would find themselves living as lesbians. Furthermore, how they looked, lived and loved needed no apology.
In summary, in the clinic we witness this toxic collision of factors: a world telling these children they are ‘wrong’; they are not doing girlhood (or boyhood) correctly. They realise their nascent sexual desire is going to be problematic; they struggle in puberty because it is uncomfortable, weird and unpredictable (particularly heightened if they happen to be on the autistic spectrum).
In all of our good-willed attempts to be empathetic, to share the pain of these very young people, we adults must not lose sight of the risk of joining too closely with them. Their pain is real, their way of making sense of it may be helpful, but it may not. Adults and professionals have a duty to step back from the feelings, whether their own or the young people’s, in order to consider what is fundamentally in young people’s interests. Listening can occur at many levels. We can hear and respond to distress without agreeing with the other person’s explanation of why they are experiencing it.
The significant treatment decisions being made are adult decisions. It is simply not possible for a child or adolescent to conceptualise a loss of fertility or sexual pleasure before they have developed their adult body.
We are dealing with strongly held beliefs and associated feelings. On the one hand is a novel belief that we are all born with an innate ‘gender identity’ but sometimes, tragically, for some trans people they are born into a sexed body that is misaligned from that gender identity. From this perspective, the problem is a tragedy of birth, as with other genetic or physical difficulties. From this position it would seem and feel as though the only sane and morally congruent thing to do is to speed up access to medical treatments. After all, if this is a medical/physical problem then, of course, a medical/physical solution will be most apt. Why would you want to hold a person back from that? However, even if this were true, there would still be many questions about the long-term trade offs of pre and post puberty ‘gender affirmation’, and different regimens and operations. Ethics would still demand high quality research into the size of harms and benefits of major medical interventions on a healthy body for a psychological indication.
On the other hand is the belief that no one has a gender identity that is discrete and separate from the rest of their identity/personality. The body we are born into is, therefore, just that. People with gender dysphoria usually exist within a healthy body, regardless of how they feel about it. From this position, the gender identity, however conceptualised, must have been formed through the developmental processes that the young person has undergone. If we believe this, then the only sane and morally congruent way to alleviate the distress is to explore their past and ongoing developmental processes in order to help them make sense of, and influence, their distressing feelings. We would consider the use of therapy to help alleviate this distress as virtually mandatory, as this is what we usually apply to distress. From this position. it would be unethical to intervene at the level of the physical body at all, as this is not the problematic feature.
When we frame the conflict in this area as being related to differences in, albeit deeply held, adult beliefs then we can also allow room from which we can compassionately relate to those we disagree with. We can see that (most) actors in this story are trying to do the best for themselves, their children or their patients, even if we think that their approach is not the right one.
Currently there is no way to distinguish amongst these children and young people, other than subjective accounts emerging within a meta culture in which even suggesting that social contexts, let alone trauma and co-morbidity, can lead to gender dysphoria is seen as transphobic.
As a final thought, the continual collapse of ’trans and gender non conforming children’ into one seamless category is highly problematic and moreover is, most likely, in part responsible for the self-perpetuating inflation of the identification of so-called’ trans kids’. Gender non conforming children are just that – not conforming with rigid social norms. In the past they might, indeed, have been labelled “tomboys” or “cissy boys” but they were not taken to professionals for “affirmation” of being wrongly “assigned” a sex at birth. Perhaps if they were left alone, and actively supported to be non conforming, this would inevitably dismantle some of the basis upon which ’trans’ is superimposed onto the presentation.
We have wondered whether the early attempts to intervene in respect of gender dysphoric children have been problematic in themselves. For example, an attempt to encourage children to play with ‘gender appropriate’ toys (or more accurately ‘sex-appropriate’: prescribed ways females and males are expected to behave) and peers, and engage in similar behaviours and activities. These might have left children feeling alienated from themselves and internalising shame / disapproval. Inadvertently, the message was exactly a ‘trans’ message – you’re not really a boy if you enjoy the things girls seemingly (and are expected to) enjoy, and vice versa.
Sadly, the present criteria in the DSM (The Diagnostic and Statistical Manual of Mental Disorders) can only exacerbate the problem:
A1: A strong desire to be of the other gender or an insistence that he or she is the other gender (or some alternative gender different from one’s assigned gender).
A2: In boys…a strong preference for cross-dressing or simulating female attire; or in girls…a strong preference for wearing only typical masculine clothing and a strong resistance to the wearing of typical female clothing.
A3: A strong preference for cross-gender roles in make-believe play or fantasy play.
A4: A strong preference for the toys, games, or activities stereotypically used or engaged in by the other gender.
A5: A strong preference for playmates of the other gender.
A6: In boys…a strong rejection of typically masculine toys, games, and activities and a strong avoidance of rough-and-tumble play; or in girls…a strong rejection of typically feminine toys, games, and activities.
A7: A strong dislike of one’s sexual anatomy.
A8: A strong desire for the primary and/or secondary sex characteristics that match one’s experienced gender.
A hypothesis is that if A2 to A6 (inclusive) is where these children start, they could look to A1 as a solution to these, and then A7 and A8 follow inevitably.
If these early presenters – and more importantly their parents, caregivers and educators – had been vigorously instructed in some basic gender / sex deconstruction, it’s worth wondering whether “trans” as a solution to childhood GD would have gained such traction over the years. Have we seen an historic iatrogenesis?
17th February 2020
Notes:
[1]: It is worth noting that we are distinguishing between sex and gender, and the distress therein. ‘Gender’ means the socially imposed expectations demanded of a girl by dint of her ‘sex’, meaning being born female. These two discrete yet over-determinedly related categories of experience interact much as the factors stated above.
A large part of the problem especially for the Tavistock & Portman NHS Trust in London has been its infiltration by Transgender lobbyists over a number of years (none of whom have ever set foot in a medical school) who demand those referred there are treated via their… ‘prescription’…
This has resulted in a continiously high turnover of clinicians who quit, citing a culture of being pressurised into descisions for patients they wouldn’t have normally taken.
The Trust has also seen lawsuits by children given that treatment who later regret their decisions….and of course those same lobbyists are blaming the Trust for that!
Thank You so much MM and AH. If You agree I would like to show Your comment to my collegue psychotherapists and to others who can influence main stream thinking about gender dysphoria in the Netherlands. For many years I feel alone in my thinking about this topic. I’m happy that I’m not a child in this times, because I also was a girl who hated to be a girl, who was waiting as a five year old that a penis would grow out of me, who hated becoming breasts en mentruation, who playes soccer far before it was normal for a girl to play soccer. How about living in the 21. century as a girl I used to be. I’m happy to be a tomboy woman, happy because psychoanlysis helped me to love the person I am en to understand why I was and why I am the girl and woman who I am, in stead of quick fit ‘treatment’ of nowadays treatment.
It would be extremely interesting to see what the referral number was for 2020 – whether the downward trend has continued, reversed or plateaued? Do you have access to that data yet?
This is the first article I’ve read that appears to be science based and because it’s Sweden, I tend to give it more credibility.
Unfortunately, in the states, the group attacking trans people are the same ones that attacked gay people 30 – 40 years ago. “Sexual orientation was a choice, they all were pedophiles, they all had been abused as children and that made them gay, They would never find love only lust..”. For that reason they don’t have a lot of credibility. Some of the comments above referring to it as madness, I don’t believe they mean the wrong direction the care has taken, but anything having to do a trans people. Most are simply pushing their religion or as part of their political culture war.
Most people of all political persuasion, don’t think there should be surgeries before they are 18 many don’t understand the chemical side of it before 18. This article filled in some of that information.
I do wish they would’ve interviewed some trans people that have been trans a long time and are perfectly happy. In fact, I find that troubling that they didn’t, that seems like some scientific method being ignored.
For the record, I was never abused, I didn’t choose my orientation, The man I’ve been married to, the love of my life, my best friend, my everything for 22 years, ….proving one of their worst lies, was a lie. Yes as we’ve aged the “lust” has faded, the love has not, just like many who fall in love and grow old together. I just don’t want trans people to be political tools for religious extremist, but I also want to make sure young people know exactly what they’re getting themselves into, even if they’re older than 18. I want them to know the science not someone else’s ideology.