The following analysis was contributed by a Canadian physician
What is Top Surgery?
Since 2015, there has been an explosion in the number of teenagers and young adults presenting with gender dysphoria in Canada and the rest of the Western world. For the first time, the majority of those presenting are observed female at birth (OFAB). This group of OFAB may identify as transmasculine but also may identify as nonbinary or a number of other gender identities. Many of these folks are considering the interventions offered by gender medicine. Some of those OFAB choose to have breast reduction surgery whereas others choose to remove their entire breasts. Amputation is final. Breasts cannot grow back.
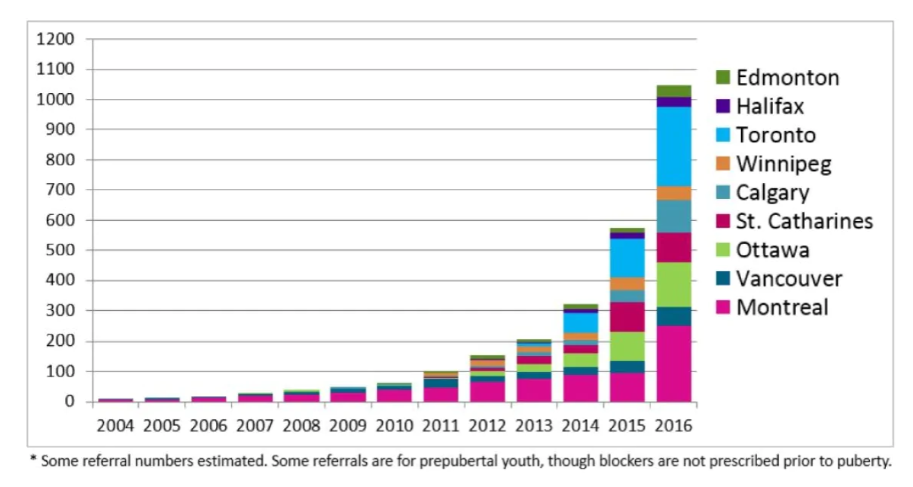
The statistic-defying numbers of young people presenting at Canadian youth gender clinics.
Source: Trans Youth Can! Study of Canadian Pediatric Gender clinics
In the world of gender medicine, “top surgery” is the term for the commonly performed breast procedures. For people wishing to appear more masculine, top surgery is generally the term for removing both breasts, also known as bilateral mastectomy. There are variations in the procedure regarding how the incisions are made and what is done to the nipples (some remove them completely to have a fully flat chest). Along with removing the breasts, there may also be a finishing touch done by removing some fat and skin next to the breast tissue, below the armpit: this is called “chest contouring”. A slim person will not have much extra tissue there, while an overweight person will tend to have more fatty tissue that can be removed. The time and cost of the supplies needed for the contouring part of the surgery is however only a small fraction of the mastectomy portion.
The potential benefits proposed to the patient wishing to have top surgery in transgender care are: being able to free yourself from wearing a chest binder (a restrictive garment to flatten the appearance of the breasts), being able to go swimming or to the beach topless, and attaining the feeling of “being your true gendered self.” Potential risks include the risks of the anesthetic and complications of the surgery, including lasting pain and numbing and reduced sexual pleasure, as well as the risk of regret if in the future the person detransitions or wishes to breastfeed a baby.
How Gender Surgeons Generate Extra Private Fees
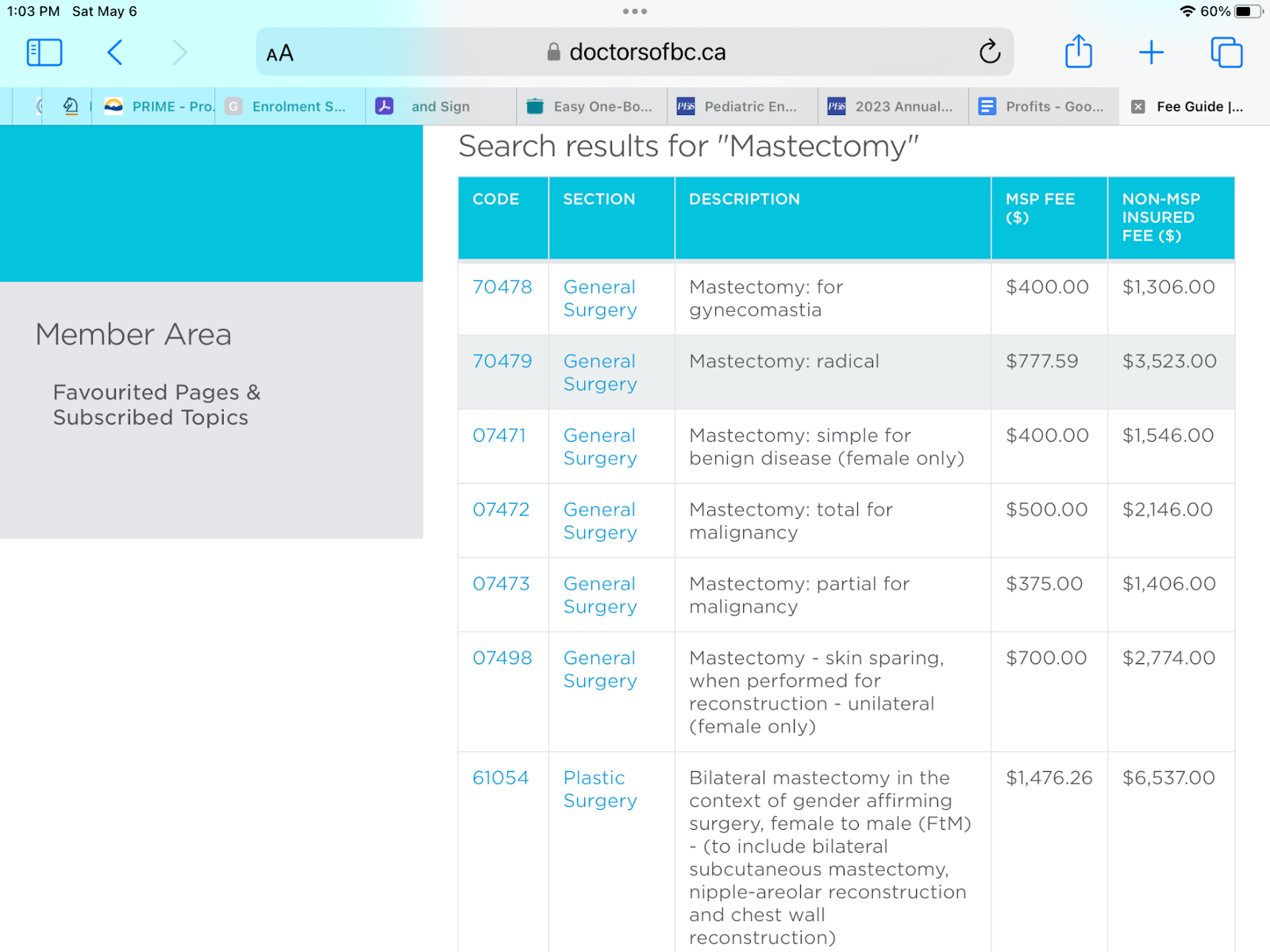
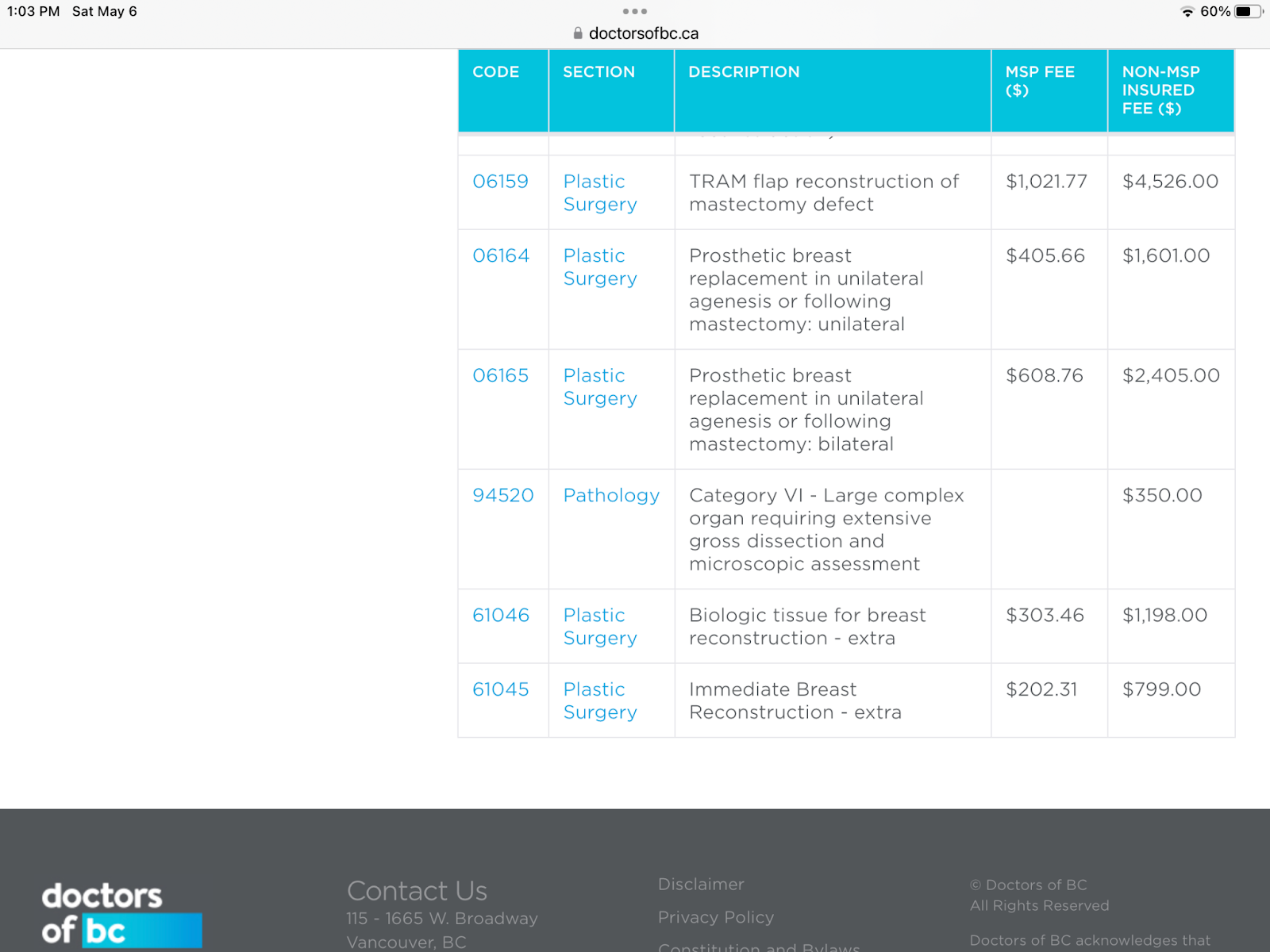
Top surgery (FTM, i.e., female to male) is becoming more popular in youth; youth in this instance is defined as 25 and younger. Although mastectomies for diseased breasts are paid for by provincial health insurance, there are often extra fees that are not covered when mastectomies are done as gender surgery. Most of the price of the uncovered service has to do with the “chest contouring” fees. The Ontario public health insurance (OHIP) does not pay doctors to do chest contouring. Some would argue that chest contouring can become a medical racket generating large private fees for what can actually be a relatively small intervention (compared to the mastectomy portion of the operation).
In Canadian hospitals, general surgeons perform most mastectomies. Most of these are for cancer. When there is a tumor, the case can be quite complex, and many variations of surgery are considered (lumpectomy with or without removal of lymph nodes in the armpit, mastectomy, or bilateral mastectomy). Some mastectomies are done where there is no known cancer yet. One such situation could arise when a patient carries a strong genetic risk with a positive cancer gene, such as Angelina Jolie. In these cases, the patient may opt to have both breasts removed. This would typically be done when the patient is not or no longer wants to breastfeed babies. Breastfeeding is impossible after bilateral mastectomy even after a reconstruction. Bilateral mastectomy was done along with a breast reconstruction in Jolie’s case. Reconstruction is complex, it can be done via breast implants or via autologous reconstruction, which is the use of either a free tissue flap (typically from the abdominal wall) or a pedicle flap (typically from the latissimus dorsi back muscle). Some women however choose to have no reconstruction done. In these cases a simple bilateral mastectomy without reconstruction can be compared to transgender surgery as it is surgically very similar to FTM top surgery. The time required for both is similar, about 2.5 hours.
How Much Does Top Surgery Cost?
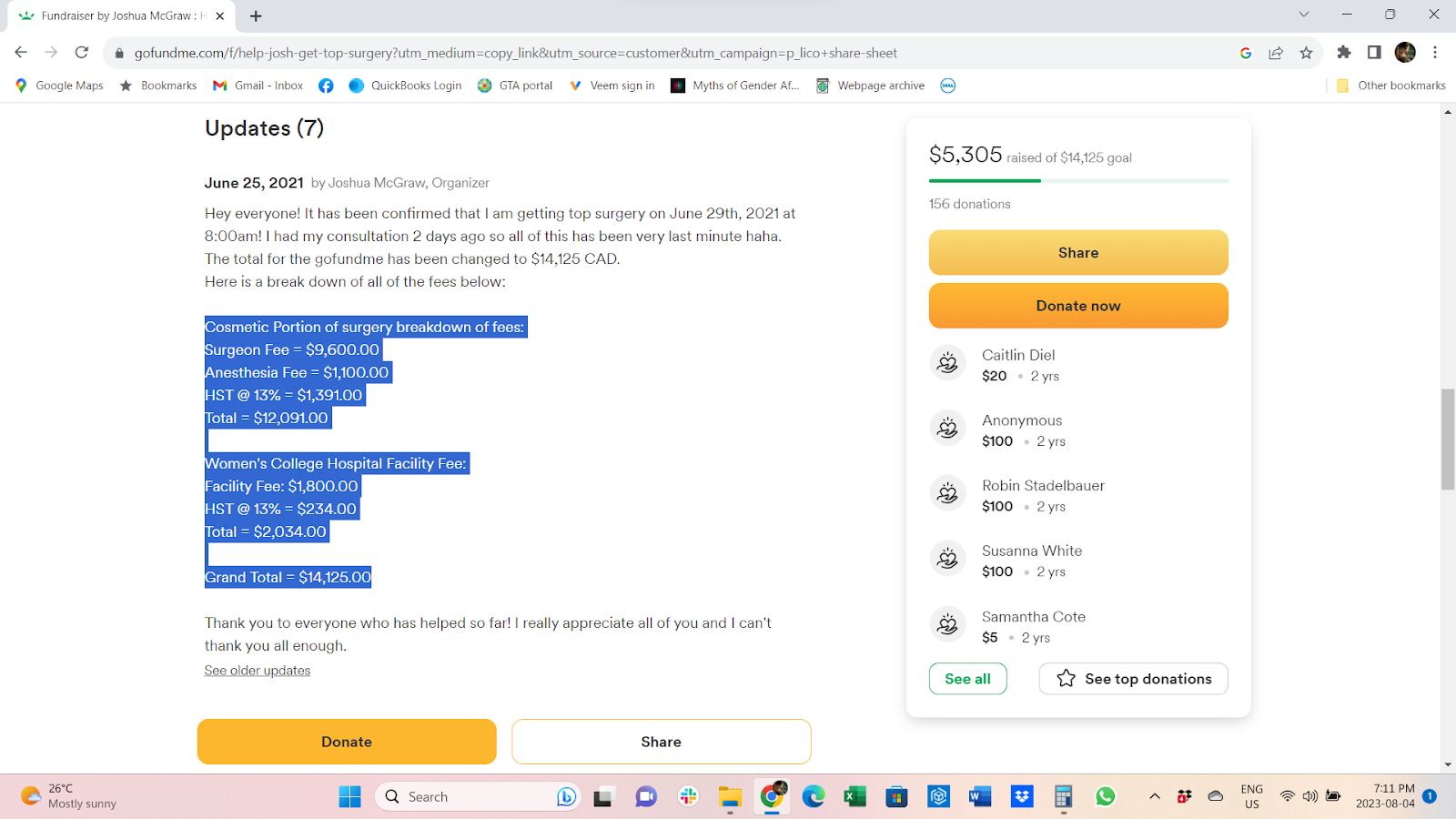
For simple bilateral mastectomies in an Ontario hospital, there is generally no need for the patient to pay extra or fundraise since required surgeries are fully covered by OHIP. However, patients having the same procedure for “gender confirmation” will often set up a Go-Fund-Me to raise between $5000 to $10,000. One Ontario fundraiser calculated needing at least $14,000 in 2021:
Where Does the Money Go?
FTM top-surgery is not more complex, not longer surgery, and requires essentially the same supplies and staff time as a simple bilateral mastectomy. Many FTM top surgeries are however done in private cosmetic surgery clinics that charge additional fees for proposed extra benefits in these fancy looking clinics.
Can we financially compare the balance sheets of FTM top surgery vs medically necessary simple double mastectomy? Accurately demonstrating all costs of medical procedures is complicated but an attempt at analysis is worthwhile to understand if these extra fees are fair. On a basic level, the costs – from the time a patient has been scheduled to meet with a surgeon to the time the patient is home after surgery – can be looked at as follows:
-OHIP (Ontario Health Insurance Plan) will cover OHIP physicians for: surgical consultation, surgeon’s operating time, anesthesiologist time, surgical assistant’s time, follow up appointment.
-OHIP will also pay hospitals a facility fee that covers nurses’ salaries, operating room equipment, medications, supplies, pathology fees, and infrastructure. Private clinics need a special arrangement if they are to have facility fees covered. Some operate without this arrangement.
-OHIP will not cover: the fees for the surgeon, assistant, anesthesiologist, and facility time for the portion of surgery that is “chest contouring”.
The surgeons in private clinics will generally continue to collect OHIP professional fees for OHIP patients having top surgery and charge them additional fees. There is usually a different fee quoted for OHIP patients and for non-OHIP patients.
In Table A at the end of this article, a bilateral mastectomy for cancer prophylaxis is compared to FTM top surgery. It is assumed that OHIP is paying the physicians when they make a claim for operating on an Ontario patient. It is assumed that a facility fee of $876 is covered in the pre-cancer mastectomy case but not in the private plastic surgery clinic (to be fair, we cannot assume that a plastic surgery clinic has been permitted to collect facility fees from the province). This facility cost is estimated from an interprovincial costing document. It is assumed that overhead office costs in all scenarios are the same. This would assume the private clinic is operating as a bare bones public system clinic. This analysis did not account for any luxury costs created by the private clinic. (That couch….priceless!)
Top Up Fees Of Thousands of Dollars
Our data in Table A shows that when patients pay a top-up fee, the potential profit available to the private clinic doing top surgery is significant. A general surgeon in the public system would get $582.76 for the care of a medically necessary simple bilateral mastectomy patient, while a plastic surgeon doing essentially the same work in a private clinic charging the extra fees could generate between $2406.27 and $7662.58 per patient as per the table below. This would be payment to the surgeon directly after reasonable expected costs (staff, supplies) of running the clinic has been paid. In a private clinic, 2 or 3 of these top surgeries could be done per day. For 3 cases, that could be $7218.81 to $22 987.74 in the surgeon’s pocket for one day’s work. Less than $2000 for the cancer surgeon and up to $20,000 for the plastic surgeon for the same day’s work.
Less than $2000 for the cancer surgeon and up to $20,000 for the plastic surgeon for the same day’s work.
These vulnerable transgender patients are essentially fundraising directly for the surgeon’s extra profit. How can this happen? Is this profiteering from vulnerable youth?
The public system gender doctors are profiting as well. Women’s College Hospital in downtown Toronto is a public hospital already receiving facility fees from OHIP, but they also charge extra for the additional “chest contouring” portion done with FTM top surgery. Contouring is currently not covered by OHIP, and so there is a $1500 +HST cost for this procedure. Who benefits from this extra fee? It is unlikely the true added cost for the average contouring time would be $1500. For 3 cases on one day, that is a $4500 bonus above what the cancer surgeries bring in. This can actually be a source of sweet extra income for the health care providers in the public system. Most other provinces work in a similar fashion as Ontario.
How many Top Surgeries are happening?
Table B below shows BC statistics on the number of top surgeries done per year in BC, publicly available on the TransCareBC website: 647 surgeries in 2021. Total numbers of Ontario top surgeries are not publicly available. One surgeon at Women’s College Hospital quoted 200 of these cases last year. How many are done in minors is not known, but several hospitals including Woman’s College Hospital surgeons have admitted doing top surgeries on minors.

- Table B, source Transcare BC. 647 breast and chest surgeries were performed in BC in 2021-2022, with over 90% of surgeries completed within 26 weeks of booking form submission (the benchmark wait time).
Wait Times for Top Surgery vs Other Surgeries
Ontario top surgery wait times are not easily available. Transcare BC however quoted that in 2021-22, 90% of top surgeries in BC were performed within the benchmark wait time of 26 weeks i.e., there is no excessive delay in getting surgery after the surgeon sees the patient and thus no discrimination. In fact, other non-gender surgeries are arguably being discriminated against. Comparing top surgery wait times to the BC public wait time registry, access to top surgery is better than: pediatric tonsillectomy (90% done by 30.9 weeks), adult tubal ligation (30 weeks), adult hernia (28 weeks), adult shoulder surgery (34 weeks), pediatric hernia (46 weeks), pediatric eye surgery (41 weeks), and adult knee replacement (55 weeks). Reference: BC surgical wait times website: swt.hlth.gov.bc.ca
Top Profits
When large profits are at stake, humans may be swayed by money. Surgeons are only human. Top surgery is a procedure that is being done on many vulnerable young people. How much is profit influencing the frequency of these surgeries? How much does it result in unethical influencing? Who is doing the influencing? How much should society care? Most of society has come to accept cosmetic surgeries being done on consenting adults; although these situations are unsavoury, we generally tolerate that cosmetic surgeons profit comfortably.
When it comes to young vulnerable people and top surgery though, the profit motive of these plastic surgeons must be questioned.
Top Surgery = Top Profits.
Further reading about gender profits:
https://www.morningstar.ca/ca/news/209487/the-financial-cost-of-being-transgender-in-canada.aspx
https://www.grandviewresearch.com/industry-analysis/us-sex-reassignment-surgery-market
Table A Ontario:
| OHIP patient, hospital pre cancer double mastectomy 150 minNo chest contouring | OHIP patient private Clinic, top surgery Assume , contouring not done | OHIP patient private clinic top surgery 16.67% for 30 minutes of chest contouring | Non- OHIP patient private clinic Top surgery Assume contouring not done | non-OHIP patientPrivate clinic + 16.67% for 30 minutes of chest contouring | |
| Fee collected from patient | 0 | 2700$e | e | 9400$e | e |
| Surgeon consult | 96.20a | 96.20 | |||
| Surgeon OR fee | 660.00b | 660.00 | |||
| Anesthetist fee | 387.25c | 387.25 | +64.55 | 387.25 | 451.80 |
| Assistant fee | 300.24d | 300.24 | +50.05 | 300.24 | 350.29 |
| Facility feee | x, collected by hospital | 786.00y | y + 16.67% | estimate 786.00 | estimate 917.02 |
| countouring | not done | ||||
| estimated canadian general surgery office overhead f | 173.93 for office costs | 173.93 | 173.93 | 173.93 | |
| Potential pre-tax take home pay for surgeon | 582.27$ g | 2406.27$ h | $2250.64 i | 7662.58$ j | 7506.96$ k |
a A035 MOHLTC https://www.health.gov.on.ca/en/pro/programs/ohip/sob/ Collected from MOHTLC Physician Services Health Insurance Act (April 1, 2023)) Ontario Ministry of Health Long Term Care (MOHLTC)
b MOHLTC code R108 x 2, includes post-op follow up, collected from MOHLTC
c MOHLTC 15.49$ per unit (7+18 units). & base units plus 4 units first hour, 8 units second hour 3 units per 15 min thereafter.
d MOHLTC12.51$ per unit (6+18 units)
e https://www.mcleanclinic.com/surgical-procedures/breast/ftm-top-surgery/ Fees stated for patients with or without OHIP. Fee is fixed regardless of how much contouring done.
f Canadian general surgeons in 2017 surveyed paid 23% overhead , 2017 CMA Workforce Survey. Canadian Medical Association
g Ontario Public hospital general surgery model. (Surgeon Consult fee + Surgeon OR fee) – Office overhead = gross pay
h Ontario Public-Private plastic surgery clinic model assuming clinic expenses are the same rate of public hospital (surgeon consult + Surgeon OR fee + Fee collected from patient) – (estimated facility fee of 876$ + estimated overhead of 173.93) = gross potential profit for surgeon prior to any profit sharing of luxury costs. Here anesthesia and assistant paid by OHIP
i In this scenario, the extra 30 minutes of work time for anesthetist and assistant is paid by patient fee
j Ontario plastic surgery clinic, fully private pay. Fee collected from patient – (Anesthetist fee estimated 387.24 + Assistant fee estimated 300.24 + Facility fee estimated 876 + Office overhead estimated 173.93) =gross potential profit for surgeon prior to any profit sharing of luxury costs. The details of any profit sharing is unknown.
k Chest contouring can consist of a range of procedures. It may require 30 minutes of extra OR time. The same instruments are used. At times liposuction and more sutures and sponges are used. An increase in all time based costs (staff and facility fees) by 16.67% could account for 30 extra minutes of chest contouring (30 minutes/180 minutes= 16.67%).
x Facility fee is variable, it includes Pathology fee, nurses fees, disposable, sutures, dressings, drains. In Canada it may be compared to a Hospital Facility fee exchanged between the provinces for cross boundary patients. Canadian interprovincial day surgery facility payment to hospital for low intensity surgery is 876$ (CIHI, CCI). Private clinics may or may not collect a facility fee. In this analysis it is presumed that the private clinic is not able to collect a facility fee.
y private clinics may or may not collect facility fee from province. Here counted as nil income and it is estimated as a cost of approximately 876$.