Canadian Gender Report is a non-partisan, non-sectarian group concerned about the medical transition of youth, the lack of evidence-based practice in our healthcare system with respect to these invasive medical interventions, the promotion of gender identity teaching in our education system and the lack of parental rights to act in the best interests of our children.
The inclusion of gender identity in Bill C-6 will have the effect of using criminal law to interfere with decision making by mental health professionals in an area which is complex and poorly understood. Countries throughout the world are reviewing the treatment of gender identity issues and questioning many practices that are currently applied in Canada. Bill C-6, in its present form, risks locking in a medicalized approach to gender identity which is not supported by evidence.
We believe that the majority of concerns about the Bill could be addressed by adding the following exemption to the overall definition of conversion therapy:
This definition does not apply to any advice or therapy provided by a social worker, psychologist, psychiatrist, therapist, medical practitioner, nurse practitioner or other health care professional as to the timing or appropriateness of social or medical transition to another gender, including discussion of the risks and benefits and offering alternative or additional diagnoses or courses of treatment.
The purpose of this amendment is to allow professional therapists to do their job and treat mental health issues in accordance with the best evidence based practice without risking criminal charges imposed by an arbitrary and uncertain line. The list of professions is taken from paragraph 241(5.1) of the Criminal Code.
Further, we call on the Canadian government to call a formal inquiry to ensure Canadian families can have confidence in our healthcare system.
Call a Formal Government Inquiry with 3 Distinct Objectives:
- An independent review of the evidence and clinical guidelines used for assessing youth with gender dysphoria, and what is known about the long-term effects on physical and mental health, including for the new cohort of adolescents and for detransitioners.
- Restrict our education system from teaching a new form of personal identity with respect to gender that erases the distinction between male and female.
- Review and update informed consent legislation including a determination of whether young people have the capacity to consent to irreversible medical interventions of this nature.
The situation in Canada has become one in which children and young people are able to access medical gender transition based on their self-determined goals under the auspices of “informed consent”.
We present a comprehensive information package about Bill C6 and what is happening in the rest of the world here:
Suggested wording changes for Bill C6
UK High Court rules puberty blockers experimental
What does the UK ruling mean for Bill C6?
The explosion of referrals to gender clinics in Canada
UK overhauls both treatment and education protocols for minors with gender dysphoria
Sweden reviewing treatment guidelines for minors with GD
Finland Issues Strict New Guidelines for Treating Gender Dysphoria
What Canadian Families Are Saying about Immediate Affirmation
What Detransitioners are Saying about Bill C-6
Suggested wording changes for Bill C6
- Change the legal language of Bill C6:
UK High Court rules puberty blockers experimental
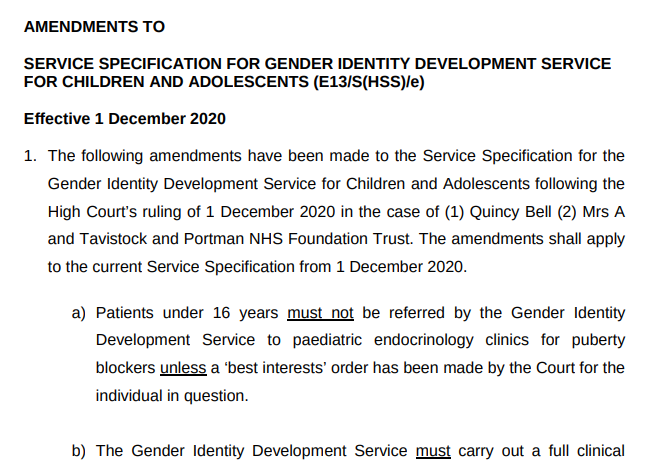
As of Dec 1, 2020 all youth require a “best interests” court order prior to being referred as a candidate for medical transition treatments at the Gender Identity Development Service (GIDS). The National Health Services issued a revised service specification for GIDS that can be accessed here. An excerpt is below:
The explosion of referrals to gender clinics in Canada
Referrals to gender clinics in Canada are following the same trend as other western countries:
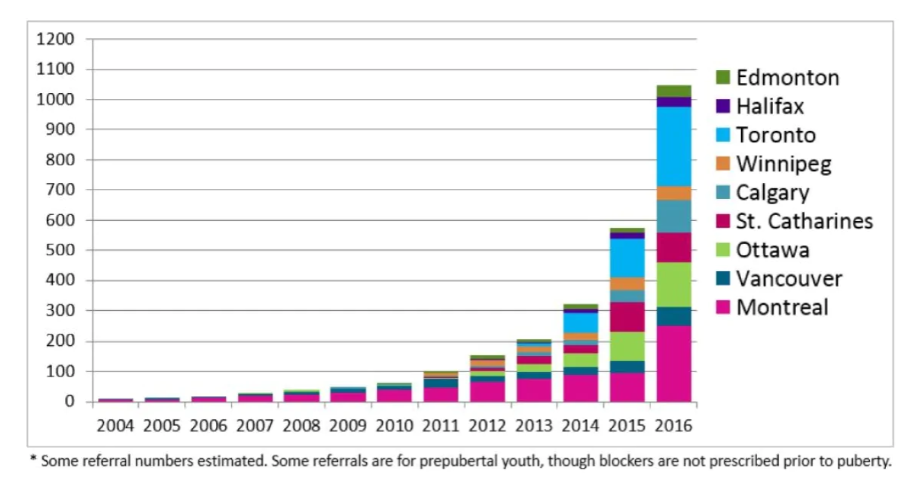
Source: Trans Youth Can!
Provincial health authorities rely on the WPATH standard of care, which is not evidence-based and for which there are growing COI (conflict of interest) concerns. See our report here. Further, CPATH (the Canadian arm of WPATH) has declared that the WPATH Standard of Care v7 is no longer acceptable because:
SOC-7 emphasizes the importance of mental health professionals’ role in diagnosing gender dysphoria and in assessing the appropriateness and readiness for gender-affirming medical treatments. By contrast, the informed consent model for gender-affirming treatment seeks to acknowledge and better support the patient’s right to, and capability for, personal autonomy in choosing care options without the required involvement of a mental health professional.
CPATH Brief to the Standing Committee on Health 2019
CPATH states that “informed consent as a model of care has evolved as an alternative to the standard model of care recommended by WPATH’s SOC”. CPATH does not make any distinction between children and adults in this briefing to the Standing Committee on Health. Also interesting is that this briefing calls out the need for banning “gender conversion therapy” and the definition found in Bill C-6 is the same as Recommendation 2 in this document.
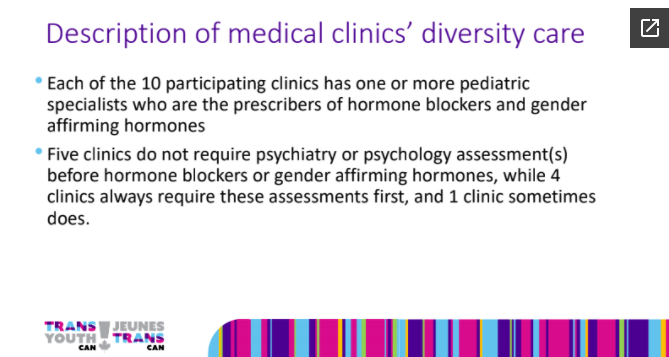
Trans Youth Can! is reporting that 5 out of 10 of Canada’s gender clinics for youth no longer require any type of mental health assessment prior to initiating puberty blockers or cross-sex hormones.
Meanwhile, in the rest of the world…
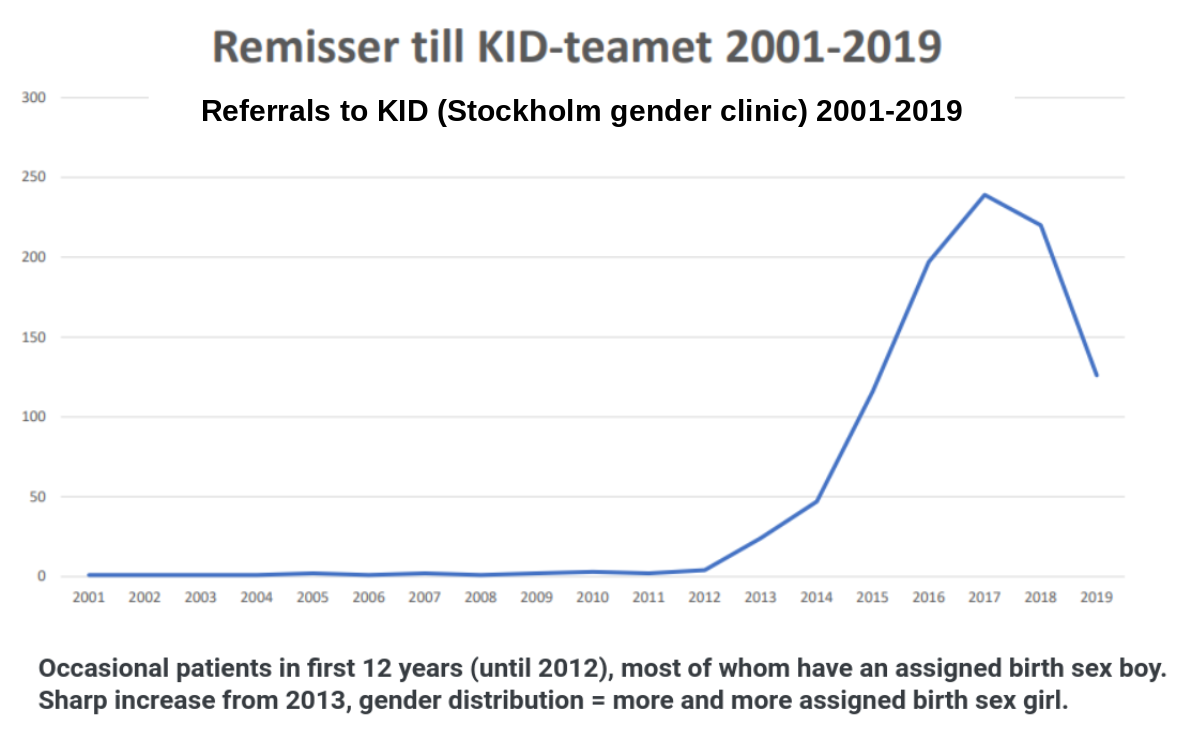
Sweden Reviewing Treatment Guidelines
Sweden, like Canada, had adopted the practice of offering puberty blockers and cross-sex hormones to children being referred to gender clinics. Until 2019. What happened? What does the Swedish experience tell us about the practice of medically transitioning children?
The Sweden National Board of Health and Welfare was tasked in 2019 to review and revise their treatment guidelines. These will be finalised 2022.
As of late 2020, only child psychiatric specialists are able to refer children to gender clinics that can initiate puberty blocking hormone therapy. The country continues to seek additional evidence to support these care standards.
A preliminary review by the Swedish Agency for Health Technology Assessment and Assessment of Social Services has not found any evidence to explain the increase in prevalence of children and adolescents who seek gender transition and “few” studies on gender-affirming treatment.
Detailed information on Sweden’s government review can be found here.
UK Calls Investigations & Faces Lawsuits
Underway now:
- Independent review by the National Health Service on the use of puberty suppressants and cross sex hormones;
- Independent review by The National Institute for Health and Care Excellence of the latest clinical evidence; and
- A lawsuit (judicial review) of the capacity of children to consent to the use of hormone blockers. [update: ruling Dec 1 requiring youth to receive a “best interests” court order prior to any referrals to GIDS or initiation of puberty blockers, x-sex hormones or surgeries]
In June of this year, the National Health Service quietly updated its website to better reflect the experimental nature of puberty blockers.
NEW STATEMENT as of June 2020:
“Little is known about the long-term side effects of hormone or puberty blockers in children with gender dysphoria.”
The UK’s Royal College of General Practitioners had stated in 2019 that “independent research into the effects of various forms of interventions for gender dysphoria is urgently needed”.
The British Medical Journal also published an analysis that concluded:
“The current evidence base does not support informed decision making and safe practice in children.”
Contrast this with Canadian public healthcare authority statements on puberty blockers:
“There are no known irreversible effects of puberty blockers. If you decide to stop taking them, your body will go through puberty just the way it would have if you had not taken puberty blockers at all.”
And “Puberty blockers are considered to be very safe overall.”
| Why are Canadian health authorities promoting hormonal therapies for children as “safe” when there is no evidence to support this statement? |
Finland Issues Strict New Guidelines for Treating Gender Dysphoria
In June 2020, the government-body Council for Choices in Healthcare in Finland (COHERE Finland) issued a number of important new guidelines for how people with gender dysphoria are to be treated in the Finnish healthcare system.
They differ dramatically from how Canadian clinics are treating gender-related distress in minors (immediate affirmation).
- Finland recognizes a clear differentiation in treatment guidelines between early-onset childhood gender dysphoria and adolescent-onset gender dysphoria.
- The Finnish guidelines acknowledge and recognize that identity exploration is a natural phase of adolescence and restrict medical interventions until “identity and personality development appear to be stable.”
- COHERE prioritizes psychotherapeutic non-invasive interventions as the first course of action “due to variations in gender identity in minors.”
- Finland recommends hormone therapy be initiated only if it is ascertained that “identity as the other sex is of a permanent nature and causes severe dysphoria” (i.e., medically necessary).
- Finland requires there be “no contraindications” or “other simultaneous psychiatric symptoms requiring specialised medical care” prior to initiation of puberty blockers or cross-sex hormone interventions.
- Finland prohibits surgical interventions for children under the age of 18
More information on Finland’s new guidelines and commentary from the Secretary General of COHERE can be found here.
What Canadian Families Are Saying
On our Healthcare System:
“I would like to clarify that it wasn’t difficult finding well-meaning gender-affirming care professionals who quickly agreed with my child that she should proceed with testosterone shots, purchase a chest binder and eventually have a double mastectomy. (This was all determined after two appointments with a psychologist and one consultation appointment with an endocrinologist at __Children’s Hospital). My child also received instant affirmation from the GP I first sought help from. That GP did not do a mental health screening or order blood tests that are usually done to rule out medical conditions that are associated with depression.
What was difficult, was finding a professional who would explore the source and severity of my child’s gender dysphoria, address her depression and anxiety, screen for common co-occurring mental health conditions order blood tests, or attempt to discuss the risks as well as the benefits of transitioning.
She did not require parental consent to start cross sex hormone injections. The result of some gentle challenge and information seeking was a teen who eventually received help for her co-occurring conditions, accepted her sexuality and now lives comfortably in her body without the need for multiple surgeries and lifelong hormone injections.”
———–
“She had recently been seeing a psychotherapist that was coaching her on what to say to Sick Kids to get hormone treatment right away. Our daughter had disclosed this to us after the third visit. Lastly, her gender dysphoria has come about suddenly with the onset of puberty at age 14 with no previous indication of gender identity issues. Our daughter denied all of this during this interview.
We left the hospital shocked at the outcome. Not feeling that a one-hour long interview with a child and ignoring all parental input and concerns was sufficient to start on a course of hormones. We never returned to Sick Kids hospital.”
On Kids Getting Caught Up In A New Trend:
A BC Mom is challenging informed consent legislation saying her daughter is “caught up in a fad”. Other experiences:
“We, to the best of our ability, just tried to understand and love our son. He was growing his hair long, had a female name and pic on his Spotify. About 6 months ago he cut his hair, cut his nails, changed his pic from a girl to no pic and changed the girl’s name back to a boy’s name. The hair cut and changes came as out of the blue as did the transgender ideas.”
“At the beginning of Grade 9 in my daughter’s high school, a new student entered who identified as transgender. Within one year, so by the beginning of Grade 10, at least six (that I know of) identified as transgender, in a class of 125. In other words, at least 5% of the grade are identifying as transgender, which is statistically improbable, if not impossible.”
“I am the parent of a teen. Born female. She now states she is in fact a boy. She “feels” like a boy. She wears “boy clothes”, (whatever that is), and has become fixated on this idea to the exclusion of any other thoughts. She has a history of poor social relationships and self-harm. Her escape has become transitioning and a near-constant immersion into Tumblr, Reddit, Mochi, Discourse, Instagram, YouTube, Twitter, and so on.”
On “Gender Fluidity” Activism In Our Public Education System:
“A few months after a school presentation by the Canadian Centre for Sexual and Gender Diversity, our son told us he was really a demi-girl. Six other children in his grade also started identifying as transgender. We had a difficult time finding a therapist who wouldn’t just affirm our son in his new identity. We finally found a therapist that figured out that our son was suffering from anxiety. After this help, he no longer considers himself a demi-girl. You’re telling us this would be a crime?”
“What happened in my daughter’s classroom was “a practice designed to change a person’s gender identity” – the very definition of conversion therapy in your Bill.” (The case of NB vs OCDSB has been granted a full hearing at the OHRT)
On criminalization of “conversion therapy” for gender identity:
“No one is arguing that transgender people should not have access to hormones or medical transition. We are advocating that for the sake of young women who are the largest growing numbers seeking medical transition, other options should ALSO be made available on an individual basis to explore and rule out other co-morbidities such as BPD, Autism, gifted intellect, gender-non-conforming so that our daughters and cousins and nieces are not directed to ONLY ONE METHOD for dealing with gender dysphoria, but permitted to grow in therapy in whichever ways seem to them individually wisest with therapeutic help.”
“Our 14-year-old teenage daughter suddenly and very surprisingly said she had gender dysphoria. This was with absolutely zero signs or indications of gender dysphoria before the age of 14. This also was two years after her telling me she was bisexual and then the next year further saying she was a lesbian. I would like to fully support her as she explores her gender identity and sexual orientation, and one of the ways that I would like to do that is through conversations with a therapist”
“Before this happened to my daughter and my family I would have been very supportive of this bill and to be clear I am in every way opposed to Conversion Therapy. After what we have been through, I do however disagree that the affirmative model of care is appropriate in all cases, especially for children. Now that I’ve been through it I can see how damaging this model can be to our young people. We are letting them down by blindly accepting their self diagnosis and not providing appropriate care and support. I’ve learned that there are so many factors that can lead to gender dysphoria that have nothing to do with having been born in the wrong body. I have learned that feelings of gender dysphoria do not last forever. I have had to navigate this on my own and with extremely little support. I feel that medical professionals, mental health professionals, and policy makers are letting families down.”
What Detransitioners are Saying about Bill C-6
Children who medically transition do not fully understand how serious and irreversible the process is. Our members often report not understanding the transition process and naively believing that their sex-change operation would resolve all of their mental health issues, and/or actually transform them into the opposite sex.
Pressure from physicians to pursue surgery:
“After about two months of taking cross-sex hormones, my physician told me that she was going to stop refilling my prescription for testosterone if I did not make an appointment with a surgeon for a double mastectomy. I had told her from the beginning that I had no plans to have either a double mastectomy or genital surgery. She persisted, though, that this was the next step in my transition.”
——
“Every time I went to speak to a doctor or therapist, they all concluded the same thing: that I was trans, and I must stay on my hormone regimen. Me wanting to desist or stop, was seen as me being unwell, and not taking my medicine. If I explained that the hormones seemed to be making my mental health worse, they would shame and coerce me into taking them again anyway.“
Bill C-6 offers no protection against homophobia:
“I knew I liked girls from a young age. I felt I was inadequate or incomplete as a lesbian. I felt I must be a man to be legitimate, or I must have male parts before I can have sex. I hated myself for being a masculine girl, a lesbian, and I felt like it was all my fault, so I would cut and burn myself, and drink heavily as a teen, to make it all go away… (This) combined with my natural gender non-conformity led professionals to assume I was a man trapped inside a woman’s body. They offered me transition, as a way to “correct” my body, instead of helping me cope with my emotions.”
Detrans Canada position on Bill C-6:
Remove the exemption in Bill C-6 for transition-related, physically-altering medical interventions (including puberty blockers, chest binding, hormones and surgical interventions) and ban those practices for patients under age 18.
For more information please consult: