
The following letter is being shared by a Canadian parent who navigated the healthcare system for the past 4 years. She cancelled that critical appointment at the gender clinic and her daughter now understands why. Some information has been de-identified. We’ve also added emphasis to highlight some key points.
This is a very extensive account and we are thankful for the diligence and steps that this parent is taking.
February 22, 2020
Dear Minister XYZ,
Thank you for your service to our province and your riding. Your hard work is very much appreciated. I am writing this letter to you because I am a parent of a child who experienced gender dysphoria from the ages of 15-18. I recognise that access for gender affirming services has greatly improved in the last few years resulting in a better quality of life for transgender individuals. Despite these improvements my child experienced gaps of care when I tried to get help for her gender dysphoria and depression in 2016 resulting in a false positive result and a referral to medically transition at the age of sixteen.
I would like to clarify that it wasn’t difficult finding well-meaning gender affirming care professionals who quickly agreed with my child that she should proceed with testosterone shots, purchase a chest binder and eventually have a double mastectomy. (This was all determined after two appointments with a psychologist and one consultation appointment with an endocrinologist at [Children’s Hospital]). My child also received instant affirmation from the GP I first sought help from. That GP did not do a mental health screening or order blood tests that are usually done to rule out medical conditions that are associated with depression.
What was difficult, was finding a professional who would explore the source and severity of my child’s gender dysphoria, address her depression and anxiety, screen for common co-occurring mental health conditions order blood tests, or attempt to discuss the risks as well as the benefits of transitioning. I naively thought my child would receive individualized care and that whatever the standard of care was for gender dysphoria it would include checks and balances for children and adolescents along with affirmative care.
My husband and I were accepting of the possibility that medically transitioning might be necessary but felt as parents we had a responsibility to ensure our teen was making a fully informed decision before consenting to irreversible chemical and surgical treatments.
It was made clear to me from the professionals my teen saw that full affirmation was the only option and my concern that my teen may also be dealing with other issues was irrelevant. My questions were acknowledged but not discussed. I was redirected to affirm not explore.
My daughter was 17 when she was seen at [Chidren’s Hospital] Endocrinology Clinic for a consultation. She did not require parental consent to begin testosterone shots at the next appointment. She had allowed me to be part of the process, so I was able to delay the next visit for a few months. When the time came for that appointment, I cancelled it after discussing with my teen my concerns about possible side effects and the need for further assessments. My husband and I did not agree with the psychologist and the endocrinologist that our child was able to give informed consent. My child was upset but luckily willing to examine some of the information that I had collected in between the time she had first told me she was not comfortable in her body (November 2015) and the two weeks before she was supposed to receive her first cross sex hormone injection (May 2017).
Initially, the information I found in newspaper and magazine articles suggested that full affirmation of a child’s gender identity and their choices to socially and or medically transition was the option with the best outcomes. Those articles often included high suicide rates in the trans population as a key reason why blanket affirmation was so important. As a result, psychologically, I began to prepare myself for the possibility that my child would both socially and medically transition. At the same time, I felt certain feelings my child had expressed to me needed to be examined further prior to beginning any irreversible procedures. In particular, I was concerned about her comment that she was unsure about her sexual orientation and had told me she was still trying to figure it out.
I didn’t care what her sexual orientation was but was wondering how that uncertainty might be contributing to her gender dysphoria. Negative comments that she had made about her appearance also suggested to me that she had unrealistic expectations of what she thought she had to look like as a teenage girl and her negative body image may be contributing to her gender dysphoria. I was also not sure if a black or white mindset was responsible for her thinking that her identity had to fit into a particular box, and she did not realise that many people do not fit the stereotypes that are linked with their gender.
I was particularly disturbed when she explained to me that she never understood why she felt different from other girls and uncomfortable with her body until she received a talk at school about sexual orientation and gender identities. I want to emphasize that I believe that talks that promote the health and safety of our LGBTQ youth are very important. I am only pointing out that perhaps the talk did not include other reasons why teens may feel uncomfortable with their bodies, such as body dysmorphia, eating disorders, not fitting gender stereotypes or a history of sexual abuse. In addition, girls on the autism spectrum or with ADHD often feel different from other girls. Unfortunately, both these conditions are underdiagnosed in females or they are assessed late such as was the case with my daughter. As a result, they do not receive the help they need in their formative years which may leave them socially isolated and wanting to find a group to fit into. (My daughter was diagnosed as being on the autism spectrum at the age of 20)
I am not implying that the presence of a co-occurring condition with gender dysphoria negates the need for gender affirming care, I am only pointing out that it makes the case more complicated and in some situations understanding the source of one’s gender dysphoria may help an individual cope without the need for severe medical interventions.
Despite mentioning these observations to the psychologist, it became clear to me that my concerns were not being addressed with my teen during the sessions. After two appointments she was referred to the Endocrinology Clinic at [Chidren’s Hospital] for a consultation.
Thankfully, the six-month waiting list bought me some time to try and find out if my concerns had any validity or was I just desperately trying to avoid losing a part of my child.
I decided to visit my local library which has a decent sized LGBTQ section. I found and read several memoirs written by trans individuals. Some individuals had decided to medically transition with positive outcomes and others had struggled with the decision and ultimately decided against it. Their reasons for not medically transitioning varied: one transman was a professional singer and did not want his voice to change, another transman was at peace with some parts of his body but not others, for several the health risks of medical interventions outweighed the potential benefits, for others living androgynously had helped them cope. One book described the experience of a transman who had given birth after temporarily going off testosterone. That author, despite chemically transitioning in his late 20’s had maintained his reproductive capabilities. Was my child less likely to have that choice if testosterone was started at a younger age? I ended up having more questions after reading the varied experiences of trans individuals who had made their decisions as adults.
Soon after my library visits, I expressed some of my frustrations about being unable to find a professional who was willing to affirm as well as explore my child’s feelings to a co-worker. Around that time (2016-2017) there had been a lot of media coverage surrounding trans rights and accounts of individuals who had successfully transitioned. I braced myself to be raked over the coals by my co-worker for not accepting that my child’s distress was simply because she was born in the wrong body and medically transitioning would alleviate that distress.
What happened instead is that my co-worker told me that she was in her early 20’s before she figured out her sexuality and accepted herself as a lesbian. As a teen she had struggled with the backlash she would get for not fulfilling female gender stereotypes. While my co-worker had never experienced gender dysphoria her partner had as an adolescent. Now in her late 30’s my co-worker’s partner was grateful that she had not transitioned and she found it concerning that the current affirmation model did not factor in the possibility that in some cases gender dysphoria could be caused by internalised homophobia or the negative feedback gender non-conforming children and teens receive from their peers.
After explaining her partner’s experience with gender dysphoria my co-worker also provided me with positive examples of friends who identified as trans. One transman had transitioned legally and medically. Her other friend was living androgynously with no medical interventions. She had kept her birth name but felt more comfortable in unisex clothing and wore a chest binder. Both individuals were living successful independent lives. After checking with each of them my co- worker generously gave me their contact info.
Several weeks later I was able to speak with one of them over the phone for nearly an hour. It was one of the kindest things a stranger has ever done for me. This thoughtful individual patiently answered my questions, gave me insight into how and why they made their decision while at the same time validating my concern that it was not a one size fits all solution.
Once again, I ended up having more questions than answers. If adults with gender dysphoria had come to different conclusions and had struggled with those decisions how could my teen be so definite about which procedures she needed.
Another reason why I was confused, was because I had no memory of my child exhibiting discomfort with her gender at a young age. Several of the accounts that I had read described preschool and elementary aged children being very expressive about being born the wrong gender.
During the times my teen was waiting to be seen at the Endocrinology Clinic I continued to address her distress and agreed that she needed help but expressed my concerns to her about the potential side effects of the treatment she had been approved for and that she needed to be fully informed so she would have realistic expectations of what the treatments could and could not do.
My feeling that she needed more education was further solidified when I came across an unrelated newspaper article. In that story the journalist had interviewed several women who had battled breast cancer and had mastectomies during their cancer treatment. The women were grateful for the surgery but wished they had been better informed of side effects such as numbness and nerve damage so they could have had a more realistic idea of what to expect post- surgery.
As a result of these side effects some of the women had become depressed even if they had not experienced depression before. My teen was depressed when she was being evaluated for hormone readiness and had expressed a desire to have a double mastectomy once she met the criteria (a year on hormones). If the psychologist had discussed the risks of surgical treatment how much could my teen have been processing in a depressed state? How could I tell if she had realistic expectations?
I was asking questions because if my teen were to go ahead with medical procedures both of us needed to be prepared to ensure a better outcome and avoid post-surgical depression. Wasn’t the whole point of providing gender affirming medical interventions to improve the mental health of trans individuals? Unfortunately, because I was asking these questions it was considered non affirming.
I continued to search for articles relating to trans issues. Along with inspirational and touching stories of individuals who had transitioned with the support of their families and communities, I was also reading about patterns that some clinicians and journalists were trying to raise awareness about with supporting data.
One subject that came up repeatedly is the increased prevalence of autism spectrum disorders found in the adolescents who were being seen at gender clinics worldwide.
This is a small fraction of what I read:
“2012 Dutch study found that the incidence of ASD among children referred to a gender identity clinic was 10 times higher than in the general population.”
“Study of the Finnish gender Identity service showed that 26% had an autistic spectrum disorder.”
“A 2017 survey of 211 de transitioned women found that 15% were on the autism spectrum, 29 times higher than the rate of autism among females in the general population”
“Autism is a risk factor for both gender dysphoria and suicidality”
As a parent who is not a researcher I could not determine the accuracy of the data that I was coming across but I discovered that Seattle’s Children Hospital has a Autism Gender Clinic in addition to Seattle’s Children’s Gender Clinic suggesting that experts in the field have established that children and teens with gender dysphoria and ASD should receive specialized care.
Clinicians who work with individuals on the ASD spectrum modify their therapy to be more experiential and concrete. In addition, all of the gender dysphoria evaluation at Seattle’s children hospital include screening for ASD. (Felice Orlich PhD, Rachel Earl PhD, Seattle Children’s Autism Center)
To further complicate matters I read the following about girls and autism from a variety of sources:
“High functioning girls with ASD are often missed by clinicians and so most of these girls had not been identified prior to being seen for their gender dysphoria”
“Girls and women with autism are underrepresented in research. As a result, we know little about how the condition manifests in them. This dearth trickles down into the clinic. They are frequently diagnosed late in life” (Dutch Project Aims to Raise Awareness of Autism in Women)
“DSMV provides some acknowledgment of differences in females and says “females without intellectual disability due to a subtler manifestation of symptoms may go unrecognised” (Dr. Judith Gould and Dr. Jacqui Ashton Smith)
“Some researchers suggest that because many people with autism struggle to find acceptance and close relationships with members of their own biological sex they start to ideate towards members of the opposite sex where they perceive more acceptance.”
“teenage girls with autism are often miserable and lonely and frequently misdiagnosed. At secondary school the become “leftover girls” drifting, alienated and often miserable lonely because the other teenage girls won’t accept them”. Guardian article April 28, 2019
“Findings in the most recent time period suggest that individuals with ASD may be at higher risk for suicide. The risk is especially pronounced among females” spectrumnews.org
“Suicide risk in females with ASD was over 3 times higher than in females without ASD” (online library)
“Females with ASD were over 13 times more likely than females in the general population to die by suicide” (Hirvikoski et al 2016 study
After absorbing this information as a parent how could I not ask why the gender affirming care my teen received did not include ASD screening especially since she was biologically female and therefore more likely to have gone undiagnosed.
High suicide rates are often quoted to promote the need for blanket affirmation but if there are equally high suicide rates found in females with ASD and there is a significant percentage of gender dysphoric youth with ASD shouldn’t an evaluation for gender dysphoria include an ASD screening before gender affirming medical procedures are approved? The hormones and surgery may help alleviate distress in someone with only gender dysphoria but how would they help someone who has both and has never been treated for ASD?
During my teen’s consultation at [Chidren’s Hospital] I expressed concern about autistic traits I had observed in my child. Instead of it being addressed the endocrinologist tapped the file containing the report from the psychologist and said, “this is all we need to go ahead”.
In that moment I felt my stomach drop and felt fearful for my child’s well- being because I suddenly realised that somehow in the case of gender affirming care the onus of responsibility that a doctor normally has when prescribing medical interventions does not apply with trans patients.
The following quote belongs to James Caspian a psychotherapist and former trustee of the Beaumont Trust (the oldest charity to work with transgender people in the UK):
“Standards of care for treatment have been hugely liberalised in a move to make things easier for transgendered people. Move is towards treatment on demand. The only way you can have treatment on demand is if doctors abdicate their responsibility of care.”
I had mistakenly thought by being referred to the Endocrinology Clinic at [Children’s Hospital] my teen would receive further psychological screening or assessments and I would have a chance to have my questions answered and be given more information with which my teen could assess if, in her individual case, irreversible life changing medical interventions would be beneficial, the essence of informed consent.
I realised during that consultation that the onus of treatment was placed on my teen who was exhibiting signs of depression and was trying to alleviate her distress which she had self-diagnosed as being solely due to her gender.
My seventeen-year-old, could consent to gender affirming medical interventions so I had no legal right as a parent to delay treatment until further screening was done. When we were given the list of potential side effects with testosterone injections, I asked if my teen could be screened for the presence of any of the blood clotting disorders that were mentioned as a risk factor. I was told the clinic would not do those tests, but we could go to a GP and request them. When we went to a GP, we were told the specialists at the Endocrinology clinic should do it.
My child never went back. As I mentioned earlier in this letter, I cancelled the follow up appointment.
It has been three years since that consultation at [Chidren’s Hospital]. My child is now twenty. She is comfortable identifying with her biological sex, she has accepted her bisexuality and is no longer depressed. A recent autism diagnosis has helped her put in perspective her social and sensory challenges.
Fortunately, she never proceeded with the irreversible treatments for which she was initially approved at sixteen.
My child is an example of how blanket affirmation is not the best treatment plan for some teens with co-occurring conditions. The lack of screening can create false positives which in turn delays treatment for those individuals whose circumstances are different and could benefit from medically transitioning.
If my child had chosen not to look at the information, I had gathered for her, and returned to the Endocrinology Clinic she would have received treatment that was unnecessary, some of it irreversible and possibly psychologically damaging if she felt she had made the wrong choice.
In addition, she would have taken the time away from someone with more severe gender dysphoria who could benefit from the chemical interventions.
I believe the professionals involved with my daughter’s case were well meaning and took her distress seriously. But her case is an example that powerful interventions need assessment. She was approved for treatments she did not require and that could have caused more harm than good. While at the same time other possibilities for her distress were not examined. This left her at risk as the suicide rates for females with ASD and females who are bisexual are high.
I was eventually able to get my daughter on a ten month waiting list for an ASD assessment. She was diagnosed in October 2019, three and a half years after I initially sought help for her depression.
Perhaps my daughter’s gender dysphoria could have been resolved earlier and she could have started treatment for her autism earlier if gender affirming clinicians in [Province] were following the standards of care guidelines set by the World Professional Association for Transgender Health which (on pg. 24) recommends that mental health professionals should screen for other mental health concerns and incorporate the identified concerns into the overall treatment plan.
Today my daughter is doing well but I am still haunted by what could have happened and feel a sense of obligation to write about these gaps in care in case there are other adolescents in [Province] receiving care for gender dysphoria that may also have undiagnosed conditions affecting their gender dysphoria.
If [Province] is similar to other Western countries cases like my daughter’s may be increasing. This is what is being reported on in other countries:
“35 Psychologists have resigned from London’s Gender Identity Development Service at the NHS foundation trust since 2016 due to concerns of gender dysphoria over diagnoses”
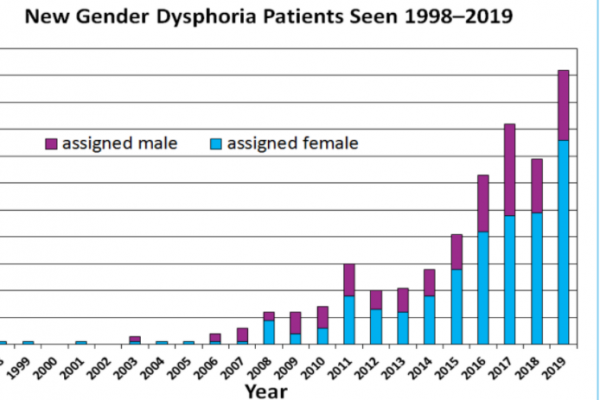
“Around 2013 something shifted dramatically, gender clinics began documenting soaring numbers of teens mostly girls seeking help for gender related stress. Adolescents claiming GD today are demographically and etiologically different from the population on which we have the most research”
“There is often a lack of focus and discussion on youth who may outgrow dysphoria and the likelihood they may be lesbian, gay or bisexual”. (Dr. Kenneth Zucker has done extensive research on this particular topic)
The following documentaries discuss the increase of cases:
The Trans Train-Swedish documentary https://www.youtube.com/watch?v=oDV-ZL6-Gu0
Transgender Regret- A Dutch Documentary February 2019 https://www.youtube.com/watch?v=1bV8AaeYKjQ
Dr. Alexander Korte a Child and Adolescent Psychiatrist in Munich, Germany was interviewed on this subject https://www.kjp.med.uni-muenchen.de/video/interview_sub_final.mp4
De transitioning: Reversing a gender transition https://www.youtube.com/watch?v=fDi-jFVBLA8
The following two quotes are from a February 22, 2020 Guardian article:
“…a report from Sweden’s Board of Health and Welfare which confirmed a 1,500% rise between 2008 and 2018 in gender dysphoria diagnoses among thirteen to seventeen year old, individuals born as girls.”
“Sweden’s authorities are starting to respond. Shortly before the bill that would have lowered the sex reassignment minimum age was due to be debated in parliament in September it was shelved, and the Board of Health and Welfare was ordered to reassess the evidence. Its report is due on March 31.” https://www.theguardian.com/society/2020/feb/22/ssweden-teenage-transgender- row-dysphoria-diagnoses-soar
At the end of the day parents just want what is best for their children.
For some adolescents with gender dysphoria that may be medically transitioning for others like my daughter their gender dysphoria may resolve without severe interventions because it is secondary to another condition. Honest attempts should be made to help both groups and standards of care should reflect that.
Gender dysphoria is a complex issue and oversimplifying it results in gaps of care leaving some groups vulnerable.
I wrote this letter in the hopes that children and adolescents seeking help with gender dysphoria in [Province] will receive care that is individualized, nuanced and more comprehensive than my daughter received to ensure that only those individuals who can truly benefit from medical interventions receive them.
My other hope is that gender affirming care for children and teens in [Province] will allow parents to freely express their reasonable inquiries and concerns without fear of being accused of being negligent or abusive caregivers.
I thank you and your staff for your public service.
Sincerely,
Name (I have not included my full name because I wish to protect my child’s privacy)
Feature image source: Photo by dashu83 – www.freepik.com

As a psychology student, this letter is incredibly insightful. The research you did, was not only beneficial for your child but also everyone else who came across this page.
As a 17 year old bio male considering going on estrogen. I found this very helpful and I believe that parents should be fully aware of what their children are consenting to. That’s why I’m every session I will request that my mother will be by my side included fully. Because as it so happens I might be on the spectrum as well (but this is not for certain) that’s why I will also be requesting a screening as well as blood work to disclose whether or not I have low iron. My current goal is to acquire as much information as possible and share as much as possible with my mother. Because at the end of the day for a lot of these healthcare professionals are either concerned with money at the cost of botching children without informed consent. Or they just want to make it an easier process. I’d like to go into this knowing what to watch out for. And I certainly don’t want it to be just me and the doctors. It should be more of a group thing rather than solely up to me.